ELBOW TENDINITIS

Treatment options for joint damage
Elbow tendon problems are some of the most frequently treated ailments seen by orthopaedic surgeons. What is unique about these elbow tendinitis conditions is that the elbow tendons sustain damage, usually from overuse, but fail to repair themselves like most other soft tissue injuries in the body usually do. The result is often a long period of time where patients expect their elbows to get better on their own, but they never do.
Lateral epicondylitis is the most common elbow tendon problem, especially in patients in their 40s and 50s. This condition is also known as
tennis elbow because 10-50 percent of tennis players experience this
condition at some point in their lives. It affects men and women
with equal frequency, and it can also be due to repetitive motion in
certain occupations such as painters, construction workers and plumbers.
Lateral epicondylitis occurs in the dominant arm 75 percent of the
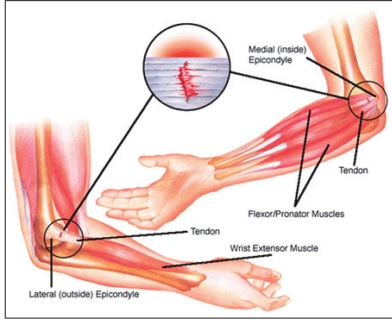
time. Symptoms of this condition are pain on the lateral (outside) part
of the elbow/forearm, pain with wrist extension, weakness of grip
strength, and pain with forearm rotation. In tennis and racquetball
players, it has been shown that improper grip size, racket weight and
racket stringing can lead to having tennis elbow.
Evaluation of tennis elbow involves a physical exam and X-rays to assess the elbow joint. Treatment is usually nonoperative and initially includes using anti-inflammatory medications, activity modification and bracing. If pain persists, cortisone injections can be used to help control the pain. Physical therapy can help accelerate recovery through the use of soft tissue treatments such as ultrasound, friction massage and dry needling.
If these treatments are not effective, a special type of injection called a PRP injection (platelet-rich plasma) is considered. This injection involves taking a small sample of the patient’s own blood, spinning the blood in a centrifuge machine, and extracting the concentrated platelet cells out of it. These cells have unique healing factors in them which are then injected into the damaged elbow tendon, initiating a healing response where it was previously lacking. Success rates of this treatment are up to 88 percent.
If non-operative treatment fails after three to six months, surgery is considered. Surgery involves resecting the damaged or abnormal portion of the elbow tendon and repairing the healthy tendon back to itself. This is an outpatient surgery which typically takes at least six weeks to fully recover from. The elbow is briefly immobilized (one to two weeks), and then motion is begun with supervision of a physical therapist. Success for this surgery is reported in up to 90-95 percent of patients.
Medial epicondylitis, or golfer’s elbow, involves pain of the tendons on the inner side of the elbow. As the name implies, this condition is commonly seen in golfers, but can also be present in throwing athletes. It typically involves men and women in their 40s and 50s and usually involves the dominant arm. Like tennis elbow, medial epicondylitis is also seen in plumbers and construction workers. Pain is located on the medial (inner) elbow with wrist flexion and forearm rotation. Irritation of an adjacent nerve called the ulnar nerve can cause burning pain or numbness/ tingling in the ring and small fingers.
Physical exam is very important in this condition to determine if golfer’s elbow versus an injury to the ulnar collateral ligament (Tommy John ligament) is present.
X-rays are done to evaluate the elbow joint, and sometimes an MRI is done to assess for a tendon tear.
Like tennis elbow, non-operative treatment involving anti-inflammatory medications, bracing, physical therapy and injections is the mainstay of treatment for golfer’s elbow. Surgical treatment may be considered after three to six months of failed conservative treatment and involves removing the damaged tendon tissue, reattaching the healthy tendon, and addressing the ulnar nerve, if necessary. This procedure is done as an outpatient and recovery is typically six weeks before resuming normal activity. Success rates are reported as 85-95 percent for this surgery. Most athletes are able to return to their normal level of competition in their sport after surgery.
Carlton Houtz, M.D., is an orthopaedic sports medicine surgeon at Highland Clinic Center of Orthopaedics and Sports Medicine, who routinely treats elbow tendinitis. He can be reached at (318) 798-4623, and his office is located at 1455 E. Bert Kouns Industrial Loop, Suite 210, Shreveport, LA 71105. Visit http://www.highlandclinic. com/staff/carlton-houtz-m-d for more information.
